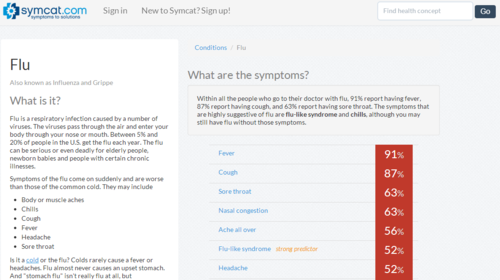
This article recently published in the Washington Post summarizes the results of a recent study published in BMJ of 23 symptom checkers. Symcat performed the best of them for diagnosis, correctly identifying the diagnosis in the top 3 listed in 71% of cases. Still, probably not as good as a doctor visit, but then again this is based on symptoms alone, no physical exam or lab tests.
Startups are hard. There’s no book. Or are there too many books? If you’re like me, you wind up feeling like you need to learn everything for yourself. That you have to “touch the stove” to know it’s hot.
It can be time consuming to learn Everything There is to Know, so instead we gravitate towards principle, heuristics, or rules of thumb. A set of heuristics are based on specific numbers–Magic Numbers. They can be used as signposts to guide decision-making where uncertainty otherwise prevails.
Several Magic Numbers frequently come up for me: 2, 3, 5, 7, 10, and 10,000. Why are they so magical? I’ll tell you.
This week I will finish the 2-part series with answers to the questions:
How did your school admin respond to your request to take a year off for your start-up?
How did you juggle the challenges of running a business with the rigor of being a medical student?
What are some of the skills/lessons you’ve learned while running a business that a typical student would never even think of?
How do you see your decision to launch a business in medical school influencing your future career (residency application, specialty choice, lifestyle, etc.)?
We were recently asked by The Doctor’s Channel to share some of our thoughts about being an entrepreneur while in medical school and how that came about. It’s not easy to take the plunge into starting a business with so much medical training already behind you and so much to go.
Here our some of my answers the the questions we are typically asked about starting Symcat while in medical school. Since there are a lot, I’m splitting it up into a two-part series. This week I will be answering
Did you have prior experience in business/start-ups before launching your own?
Before you started medical school, did you have any feeling that you would be starting a business while still in school?
At what point did you start thinking your idea could be scaled from just your school to medical schools across the US?
Can you tell me how you made the tough decision of taking time off from school and the different pros/cons you weighed?
In an effort to offer more data driven tools to patients and providers, we have released our new heart disease risk calculator.
The tool implements the algorithm presented in the new ACC/AHA guidelines on the assessment of cardiovascular risk. The guidelines and companion algorithm have gotten a lot of attention recently mainly for suggesting that many more people should be on statins and for changing the way LDL is used for titrating these medications.
In addition to calculating the 10-year risk of heart disease and stroke, we also incorporate the recommendations from the same guidelines for when to start statin therapy.
The calculator is still a work in progress and we welcome your suggestions about how to improve it. In time we will be integrating this fully into the Symcat dashboard functionality along with other predictive algorithms.
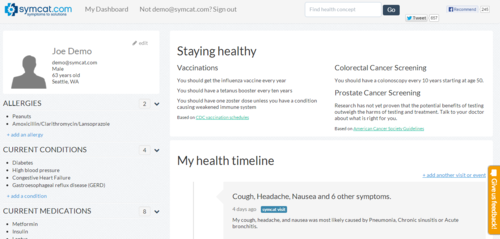
Great news for our awesome Symcat users: We’ve added a bunch of new features that you can read about below. We recommend poking around the site to explore the new features for yourself. As always, please give us feedback so we can keep working to make Symcat the best resource out there to take control of your healthcare.
Our new features make it easier than ever to:
Check symptoms: Figure out what conditions you might have with Symcat’s simple wizard. With over 200 smart decision points in the questionnaire, the Symcat lets you quickly narrow down the list of possible diagnoses and decide on the next step for care.
Find providers: Compare the cost and quality of providers in your area or across the nation. Find out where to go to for a specific procedure and research what providers are likely to charge. (More to come in the next few days!)
Learn about medical concepts: Educate yourself on conditions, symptoms, and treatments that are relevant to you. Symcat has all the info you’re looking for in a format you can use. Find out what a treatment entails, learn about side effects from your medications, or just prepare yourself for your next doctor’s visit by reading up on your condition. If you’re looking for examples, why not check out cough or diabetes?
Manage your health: Skip many of Symcat’s questions the next time you experience symptoms by creating a Symcat profile. With a profile, you can use Symcat’s dashboard to record symptom episodes, identify preventative care that’s tailored to you, and find care more quickly in the future. And of course we don’t share your data with anyone without your consent.
Give the site a look, send us feedback, and stay tuned for more updates!
I was absent-mindedly playing with my iPhone today and took special notice of a feature I have rarely used before. If you swipe all the way to the left on the home screen, you will get a search bar to search all of your iPhone. This includes contacts, iMessages, and apps. I’ve never needed to use this before–a testament to the iPhone’s ease of use. Just prior to this, I was working on some patient notes using my hospital’s electronic medical record (EMR). In contrast, each task I performed required a highly-regimented, multi-click process to accomplish.
Criticizing EMR interfaces is a well-loved pastime among clinicians. Here, however, I am going to take an oblique approach and reflect instead on what has made good interfaces (all outside of medicine, it turns out) recognized as such.
I searched for the term on popular healthcare blogs and found the following meanings from doctors. They want:
The ability to obtain outside records.
To avoid redundant entry of information
A single login for different applications (e.g. the applications that control scheduling, patient location management, inpatient documentation, outpatient documentation, order entry, and radiology display)
To compile information from different databases and hardware devices like heart monitors and EKGs.
When I read publications from the ONC and the “thought leaders” who write on this topic, I hear terms like SNOMED, ICD-10, HL7, OSI, secure messaging, and so on.
Am I missing something?
Conversations between the government and industry leaders have misconstrued the problem’s complexity and over-engineered its solution at great expense. They fail to listen to physicians, who are simply complaining that they cannot get records from outside their health system.
I am frequently asked about the “A-ha” moment that led to the creation of Symcat. This is frustrating because I usually have to make something up about an apple falling on my head or a dream about a snake. People generally think of ideas as spontaneous, as not existing one moment and existing the next. But Symcat has taught me that they are wrong.
I applaud the New York Times for elucidating the incentives that underlie adoption of EMR systems in large medical centers [1]. Bob Wachter wrote a critical piece arguing that Meaningful Use incentives were necessary–that the adoption curve for EMRs is the absolute measure of improving patient care [2]. I want to give the perspective, as a student of medicine and technology (and a daily user of hospital EMRs), that the five major EMRs that now hold control of 50% of our major medical centers and a similar amount of our patient data are unlikely to deliver on promises to improve the quality of patient care [4]. This is due, in part, because Meaningful Use has failed to emphasize the importance of design and open data in health information systems.